
Diagonal earlobe crease (DELC), also known as Frank’s sign, is a physical characteristic often associated with coronary artery disease (CAD). This article explores the diagnostic accuracy of using a diagonal scan tool, essentially a visual assessment of DELC, for detecting CAD. We will delve into the research surrounding Frank’s sign, examining its potential as a diagnostic indicator and its limitations.
The History and Physiology of Frank’s Sign
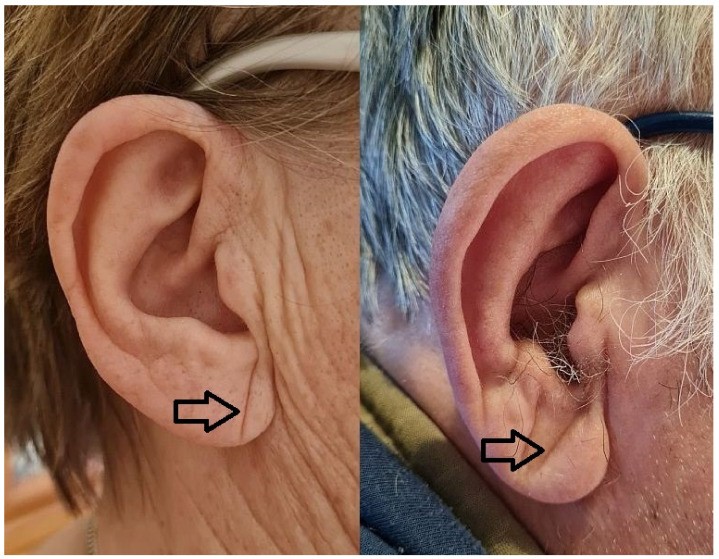
Frank’s sign, named after Dr. Sanders T. Frank, refers to a diagonal crease extending across the earlobe, typically from the tragus towards the lower edge. First described in 1973, this visible feature has been linked to atherosclerosis, the underlying cause of CAD. While the exact physiological connection remains unclear, several theories propose that DELC might result from:
- Myoelastofibrosis: Research suggests that DELC-positive individuals exhibit myoelastofibrosis in the earlobe’s arterial vessel, potentially indicating a systemic vascular issue.
- Fibrosis and Nerve Degeneration: Studies have observed fibrosis and Wallerian-like degeneration in the peripheral nerves of earlobes with DELC.
- Chronic Hypoxia-Reoxygenation Injury: The earlobe’s unique prenatal development might make it susceptible to injury from chronic hypoxia related to atherosclerosis.
- Aging and Collagen Degradation: DELC could also be associated with natural skin aging processes, collagen degeneration, and even telomere shortening.
Diagnostic Accuracy of Diagonal Scan Tool
Numerous studies have investigated the relationship between DELC and CAD, employing invasive coronary angiography (ICA) or computed tomography angiography (CTA) as the gold standard for diagnosis. However, the diagnostic accuracy of a diagonal scan tool, simply observing the presence of DELC, remains controversial.
A review of 13 cross-sectional studies involving over 3,951 patients revealed:
- Sensitivity: Ranged from 26% to 90%, indicating a wide variation in the diagonal scan tool’s ability to correctly identify individuals with CAD.
- Specificity: Varied from 32% to 96%, reflecting the inconsistency in correctly identifying those without CAD.
- Positive Likelihood Ratios (LR+): Mostly below 2, suggesting a limited increase in the probability of CAD if DELC is present.
- Negative Likelihood Ratios (LR-): Mostly above 0.5, indicating a minimal decrease in the probability of CAD if DELC is absent.
These findings suggest that relying solely on a diagonal scan tool for CAD diagnosis is insufficient. The low LR+ and high LR- values demonstrate that DELC presence or absence does not significantly alter the pre-test probability of CAD.
Limitations and Considerations
The research on Frank’s sign has several limitations:
- Heterogeneity in DELC Definition: Studies use varying criteria to define a “positive” DELC, making comparisons and meta-analysis challenging.
- Study Population Bias: Many studies focus on patients already suspected of having CAD, limiting the generalizability of findings to the broader population.
- Confounding Factors: Age, ethnicity, and other health conditions can influence DELC presence, potentially confounding the relationship with CAD.
Conclusion
While the diagonal scan tool, or visual assessment of DELC, holds some historical interest and potential as a quick and non-invasive screening method, its diagnostic accuracy for CAD remains limited. Frank’s sign should not be used in isolation for diagnosis. However, given its simplicity, it could be considered as one factor among many in a comprehensive cardiovascular evaluation. Further research with standardized DELC definitions and broader population samples is needed to clarify its role in CAD risk assessment. A physician should always be consulted for any health concerns related to cardiovascular disease.
